This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc. and Sanofi.
Copyright © 2019 Med Learning Group. Built by Divigner. All Rights Reserved.
CRSwNP is a chronic condition that can be managed with proper treatment to reduce symptoms and improve quality of life.1 Successful management of the disease may require multiple therapeutic interventions and long-term treatment to prevent recurrence.1 Treatment options include nasal saline irrigation, intranasal corticosteroids (INCS), functional endoscopic sinus surgery (FESS), corticosteroid-eluting sinus implants, and biologics.1
Nasal saline irrigation is a part of first-line therapy for patients with CRSwNP that improves mucociliary function by flushing out mucus, inflammatory debris, and allergens.1 The treatment poses few risks if performed properly.2 Patients should be advised how to clean irrigation devices and to use distilled, sterilized, or boiled water to avoid infection.1,2
Intranasal corticosteroids (INCS) are a first-line treatment option for CRSwNP and a cornerstone of maintenance medical treatment.1,3 INCS can lead to significant improvement in symptoms in most patients, reducing polyp size and increasing nasal airflow.4
There are a variety of delivery systems for INCS including sprays and an exhalation-driven delivery system (EDS).1 Proper technique when administering INCS is necessary to achieve the maximal therapeutic effect.1
INCS sprays are generally well tolerated, with irritation of the nasal mucosal sometimes leading to epistaxis.1 On rare occasions, nasal septum perforation can occur.1 The risk of these adverse events can be reduced by using the lowest effective medication dose and ensuring proper delivery technique.1 Note that standard INCS sprays do not always reach target areas of the nasal cavity where polyps form.1 If initial treatment with INCS spray does not provide adequate relief, consider adjusting treatment to a different delivery method, such as EDS.1
The EDS device consists of a sealing nosepiece and flexible mouthpiece that administers medication as the patient exhales.4 EDS may be more convenient for patients who travel frequently and may be preferred by patients with eustachian tube dysfunction who have increased symptoms with irrigation.1

Side effects of INCS via EDS include epistaxis, nasal septal ulceration, and reddening of the nasal mucosa1. Patients using EDS should receive annual eye exams to monitor for glaucoma and cataracts, since medication delivery close to the orbit may increase the risk of these conditions.1 Consult a patient’s ophthalmologist before using EDS in patients with a history of these diseases.1
Patients with severe nasal blockage, severe nasal congestion, or anosmia may benefit from a short course of oral corticosteroids (OCS).1 Although these medications can effectively reduce the size of nasal polyps, they are not recommended for prolonged use due to the significant burden of adverse effects.1 Rare but serious side effects can occur with short term OCS use including hyperglycemia in people with diabetes or prediabetes, mood changes, and arrythmias.1
Corticosteroid-eluting sinus implants are an in-office treatment option for patients who have recurrent nasal polyps after surgery.3 The sinus implants allow for localized medication delivery and are generally well tolerated3. In a prospective cohort of CRSwNP patients who received corticosteroid-eluting sinus implants, two cases of acute sinusitis were reported3. There is a lack of expert consensus on the use of this treatment.3
Biologics for CRSwNP are monoclonal antibodies that target specific inflammatory pathways and can be considered in patients who have type 2 inflammation7 . Biologics may be considered as an alternative to surgery for patients who have contraindications for surgery, a strong preference against surgery, or comorbidities such as asthma that could also be treated with a biologic.1
Three biologics have been FDA-approved for CRSwNP: dupilumab (anti-IL-4/13), omalizumab (anti-IgE), and mepolizumab (anti-IL-5).1,6 In addition, benralizumab (anti-IL-5), reslizumab (anti-IL-5), and tezepelumab (anti-TSLP) are currently being studied as additional biologic options for CRSwNP.1,6 These are currently FDA-approved for severe asthma, but more studies are needed to determine their effectiveness in CRSwNP.1,6-15 The risks and benefits for each biologic therapy vary due to their differing mechanisms of action.3

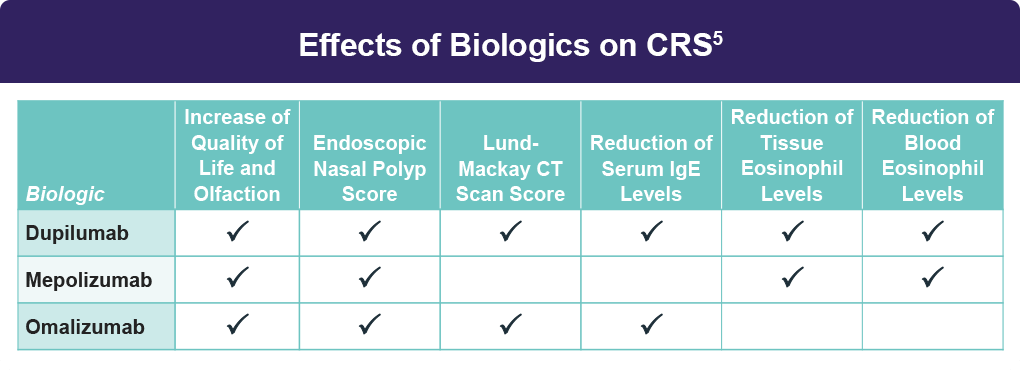
Currently there are no guidelines for which biologic should be used first and direct comparisons are needed.5 Considerations for starting biologic therapy include3:
The success of a biologic treatment should include both clinician- and patient-reported outcomes10. Proposed reasons to continue biologic therapy once started include improved quality of life or >50% reduction in systemic corticosteroid use without additional surgery.3

All URLs accessed on 8/26/24.
This activity is provided by Med Learning Group.
This activity is supported by an independent medical education grant from Regeneron Pharmaceuticals, Inc. and Sanofi.
Copyright © 2019 Med Learning Group. Built by Divigner. All Rights Reserved.
